Should I have My Leaky Mitral Valve Repaired?
A leaky mitral valve, known technically as mitral regurgitation or mitral insufficiency, often requires mitral valve repair or replacement to stop the leak. It’s a no-brainer to fix the leak when it is severe and symptomatic and it is causing shortness of breath and heart failure. So you should proceed as long as your heart’s pumping function hasn’t already deteriorated too much.
When to Do Mitral Valve Repair if You Have No Symptoms
On the other hand, when you have no symptoms from a severely leaky valve, deciding on mitral valve surgery is a lot more complicated. Sometimes if you delay the repair of severely leaky valve, your heart will get bigger and weaker until it passes a point of no return and it is too late to fix it. In such cases you may suffer a progressive downhill course. This can happen silently while you have no idea that the deterioration is occurring. So it is very important for the you and your doctor to watch very carefully and do surgery at the right moment.
The most well accepted criteria for operating on minimally symptomatic or non-symptomatic patients with severe mitral regurgitation are based on echocardiography. When the echocardiogram shows that the diameter of the heart at the peak of it’s contraction is over 55 mm, or when the heart’s pumping ability falls below normal with a diameter of just 40 mm, surgery is definitely recommended.
Mitral Valve Repair or Replacement?
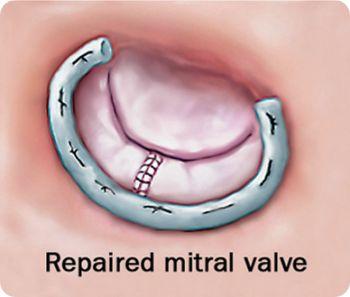
There are two ways to fix a leaky mitral valve surgically. The easiest and least technically difficult is to cut out the leaky valve and sew in an artificial one made of animal tissue or man-made material. The other option is to repair the patient’s own valve. Mitral valve repair is much more technically difficult and requires lots of surgical experience to obtain a high success rate (over 90%). The mitral valve repair option is much preferred because it leads to better long term outcomes. Another advantage is that a repaired valve does not require blood thinners in patients with normal heart rhythm. However, mitral valve repair is not feasible for some kinds of valve conditions, such as rheumatic deformities and very calcified valves.
Repair Sooner or Later?
Some surgical centers will aggressively recommend early mitral valve repair on just about anyone with severe mitral regurgitation, even when the heart has not gotten enlarged and the pumping function is still normal. Other more selective centers will take into account other early signs of heart malfunction such as irregular heart beat (atrial fibrillation) or excess pressures on the right side of the heart (pulmonary hypertension).
Many surgical centers take an aggressive approach toward early prophylactic mitral valve repair. However, there are very good clinical studies that show that if one very carefully monitors patients with regular cardiology visits and echocardiograms, that surgery can be safely deferred until the more strict criteria for surgery are met. In one study, 78% of patients could defer surgery for 4 years or more, and still have the same outcome as those who had early surgery. In other words, there is no penalty for watchful waiting.
Mitral valve surgery is far safer today, with far better outcomes than ever before, but there will always be some unexpected deaths, disabling strokes, and life-threatening infections. Sometimes attempts at mitral valve repair fail, and the patient is left with a leaky valve or must have repeat surgery to put in the less advantageous artificial man-made valve. It’s impossible to predict in advance who will fall victim to these complications.
So as safe as surgery is today, the cardiologists in our practice prefer not to recommend early surgery in non-symptomatic or minimally symptomatic patients who have not yet met clear criteria for mitral valve surgery. We believe that early surgery exposes patients to the risks of operation sooner than necessary. If as good studies suggest, there is nothing to be lost by watchful waiting, then months and years of good quality life can be guaranteed rather than chancing a serious complication earlier rather than later.
What if I Am Too High Risk to Undergo Mitral Valve Surgery?
Other new less invasive options such as the MitraClip may be offered to patients who are too frail for heart surgery. This technique uses catheter delivered instruments that are passed from the groin without surgery to reduce the mitral valve leak. The MitraClip attaches the two mitral leaflets together to reduce the leak. For some patients who are very high risk surgical candidates, this approach can be a reasonable option, but the success rate is much poorer than with surgical repair.
When deciding on whether to have your leaky valve fixed, it is important to understand the orientation of your cardiologist and surgeon on the question of early prophylactic repair of your leaky mitral valve.